MSK toolkit: Point of referral and patient journey
MSK tookit
Theme 1: Point of referral and patient journey
MSK podiatry services exist in many forms throughout the NHS and regional provisions vary. This appears to be based on relationships with community and acute trusts, primary care networks and historical contracts that are repeatably renewed. Often, change is limited to how proactive individual management and commissioners are in altering the MSK service provision. Having a suitable mandate with guidance to improve and amend care gives MSK podiatry team leaders leverage to alter existing systems to enable faster and more efficient care.
When evaluating the patient’s journey to gain access to the appropriate level of podiatry MSK care, either within the community or acute trust, on average one or two other practitioners are consulted. Athough, when a First Contact Practitioner (FCP) is working in primary care in a GP’s surgery, this journey is reduced as immediate contact with the podiatrist is made first time. From the referral source to podiatry, the average time for a patient to be seen by MSK podiatry is between 3-8 weeks. Then, after initial contact and assessment are made, the average patient receives two appointments (an assessment with initial treatment followed by a review with discharge). In some cases, depending on pathology, this can be longer and with paediatric cases where care can be ongoing until the patients are 18 or deemed suitable to discharge. Once a patient is assessed and treated, there is an average period of between 8-14 weeks for the patient to be discharged completing their care. Again, this is not the case observed for paediatric cases and when treating complex complaints, it is acknowledged that patients can continue their pathway of care indefinitely.
Patient journeys do vary within geographical localities, however once a patient has been seen by MSK podiatry, a common theme of treatment includes assessment and initial intervention at first appointment with a review and possible discharge at second appointment. In some cases, the patient is referred into another service (physiotherapy/orthotics and surgical intervention (podiatric or orthopaedic)). Other pathways of care lead patients to diagnostic testing/phlebotomy/casting for bespoke device and other healthcare services, including mental health, chronic pain and dietetics.
Referrals into an MSK podiatry service can be via the GP, self-referral or by another medical/ healthcare professional. Within the tiers of care, there may also be a referral route from a FCP into community and multidisciplinary team (MDT) services as appropriate as well as referral between the podiatrists working in community and MDT hospital settings (Figure 1).
It is acknowledged in this report that completing the correct initial referral into services can be the main hurdle to access care; therefore, there is a case to provide a national programme to raise awareness of MSK podiatry skills and engage with national workstreams like GIFRT and BestMSKhealth initiative [5,6]. The knowledge and understanding about the scope of MSK podiatry practice is frequently reliant on historical experiences, active management of services as well as relationships between departments. If these connections are weak, or relationships poor, then often appropriate referrals are mismanaged into other services which can lead to a long route for patients into MSK podiatry.
Figure 1 Referral pathways between MSK podiatry services as well as access routes into services. Where AHP= Allied Health Professionals, GP= General Practitioner. Nursing includes health visitor and district nursing. Body icon is a self-referral. 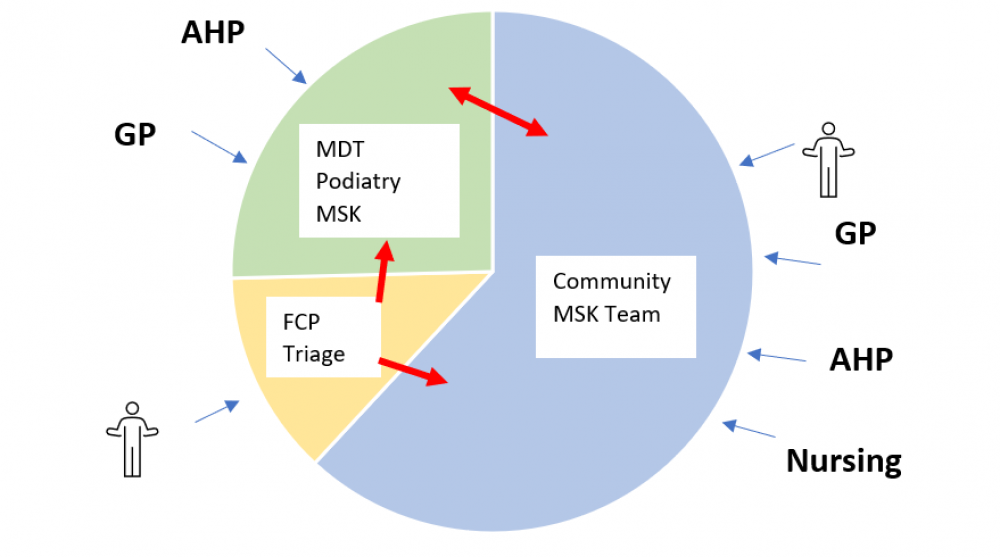
Notes:
5 Getting it right first time GIRFT https://www.gettingitrightfirsttime.co.uk/
6 BestMSKhealth programme via ARMA http://arma.uk.net/bestmskhealth-programme-launch/